
Majority of the gym population love squats and they should, squats are a GREAT exercise. However, often these people use improper form and could be doing more harm than good. The inability to squat either at all or with proper form could be characterized by the incompetency of a variety of factors. According to Myer and colleagues (2014), these factors may include: neuromuscular impairments, weakness and/or asymmetry of the muscles, instability of the joints, and/or immobility of the joints. In this article, I am aiming to describe some of the more prevalent compensations that occur with a squat pattern and explain how and why they occur.
Improper Spine Postion Complications/Implications
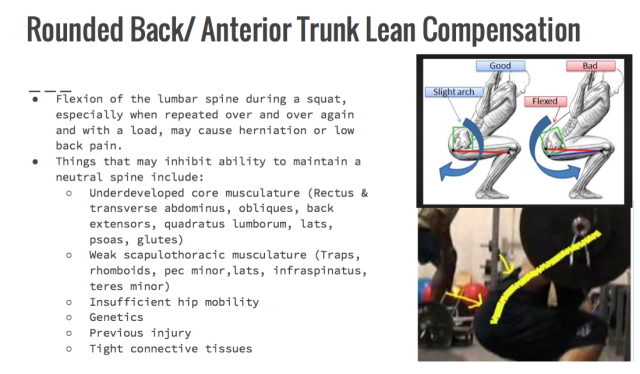
One of the most common movement pattern deficiencies for a squat is the inability to maintain a neutral spine during a squat. This can be an issue because repetitive lumbar flexion, especially under stress of external load, can lead to low back pain, herniation and other nerve-related problems. The reason this occurs is because when the lumbar spine is flexed, it causes the anterior portion of the harder vertebral discs to come together while pushing the softer, jelly-like intervertebral discs posteriorly (or posterolaterally in some cases) which then compresses the nerves in the spine and causes pain, numbness, tingling, etc. This effect is even more harmful when external weight is applied because it further increases shear and compressive forces on the lumbar spine (Kritz et al., 2009; McGill, 2010; Myer et al., 2014). Also worth noting is that further damage may occur if the lumbar spine is hyperlordotic (low back is extra-arched) or the thoracic spine is hyperkyphotic (upper back is extra rounded). According to Kritz and colleagues (2009), too much lumbar extension with an external load greatly increases the compressive forces on the spine. Authors suggest that only 2 degrees of extension past neutral can yield an increase of compressive stress increase of 16% (Kritz et al., 2009). Research suggests that this may be particularly important because findings conclude that weightlifters “hyperextend to a significant degree when lifting heavier loads” between 60% and 80% 1RM (Kritz et al., 2009).
Excessive lumbar flexion and extension and thoracic flexion during a squat could be a result of one or a combination of several kinematic deficiencies including: underdeveloped and/or underactive core and/or scapulothoracic musculature, lack of hip mobility, genetics, previous injury, and/or tight connective tissues (Myer et al., 2014). Lack of core development (rectus and transverse abdominus, obliques, back extensors, quadratus lumborum, latissimus dorsi, psoas, glutes) may lead to instability of the spine and allow more freedom for excessive flexion or extension. In addition, weak scapulothoracic muscles (traps, rhomboids, pec minor, latissimus dorsi, infraspinatus, teres minor) might contribute to increased kyphosis of the thoracic spine and thus further flexion of the lumbar spine. Maintenance of core and scapulothoracic musculature should be included in many, if not all, training programs to reduce the risk of low back injury and maintain the neutral spine.

Hip Hinge Compensation/ Implications
Another typical squat compensation seen across gyms all over the world is the lack of hip hinge during the descent portion. According to Czaprowski and colleagues (2012), this compensation occurs when the squat pattern is initiated by activation of the quadriceps and movement at the knee joint rather than the posterior chain. This inability to posteriorly shift the weight may either be a result of or lead to overactive quadriceps and underactive hip extensors (hamstrings, gluteus maximus) also described as one being quad dominant. The inability to hip hinge may lead to compensation and/or injury in other areas of the body including the knees (to be described in greater detail later in the article) and lumbar spine as well as poor hip mobility.

Forward Knee Compensation
Knees falling forward during a squat can increase shear and compressive tibiofemoral & patellofemoral forces at the knee (Escamilla, 2001). Most researchers agree that knees going slightly, but not excessively, past the toes are normal, safe, and necessary to complete a proper squat (Kritz, et al., 2009). This is especially true if the person is very tall and may have longer limbs. However, research has also suggested that if the knees remain posterior to the toes during a squat, anterior lean of the trunk may occur and cause problems for the lumbar spine (Kritz et al., 2009). Further research needs to be done to quantify optimal knee placement relative to the toes in the sagittal plane during a squat and find a happy medium for this concept. Based on current research, we have concluded that knees going very slightly past the toes may be optimal for injury prevention during a squat.
The forward knee compensation might occur due to underdevelopment and/or insufficient activation of the posterior chain (hamstrings and glutes), which then causes the quadriceps to take over the workload.

Forward Knee Implications
Research suggests that excessive tibiofemoral shear and compressive forces in addition to excessive patellofemoral compressive stress may lead to injury of the knee (Czaprowski et al., 2012; Escamilla, 2001; Myer et al., 2014). Excessive tibiofemoral shear forces can lead to injury of the ACL, while excessive tibiofemoral compressive forces may be harmful to the menisci and articular cartilage (Escamilla, 2001). In addition, excessive compressive forces of the patellofemoral joint may result in osteoarthritis and chondromalacia. When the knees fall too far forward, the excess shear tibiofemoral forces pull the tibia anteriorly and place stress on the ACL. However, when posterior weight shift and proper knee alignment (no valgus collapse) is achieved the hamstrings and adductors are stretched and oppose the shear anterior tibiofemoral forces. This results in equal force distribution of the knee joint and reduces risk of injury. Excessive compressive forces to the tibiofemoral and patellofemoral joints cause the bones to push towards each other and grind on important anatomical structures inside those joints like the articular cartilage and the meniscus that keeps the bones from rubbing against each other. Over time this can put too much wear and tear on these structures and lead to injuries.

Valgus Collapse Compensation & Implications
Valgus collapse is characterized by collapsing of the knees together and may be a result of several factors. First, it might be caused by underdeveloped/underactive hip abductors, external rotators and glutes and/or overdeveloped/overactive hip adductors and internal rotators. A second possibility is that it could be caused by a lack of ankle dorsiflexion due to tight or overactive plantarflexion muscles. Another thing that could be causing this compensation is overpronation of the ankle, which is characterized by overactive inversion muscles and underactive eversion muscles. Last but not least, neuromuscular deficiencies could be the underlying problem for this compensation. People can squat for years with incorrect form and train the motor programs to work improperly, thus needing to be retrained to keep the knees from falling inward. Some implications of valgus collapse include knee pain, IT band syndrome, and ACL tears.

Heels off the Floor Compensation & Implications
Many things may cause the heels to lift of the floor at the bottom of the squat. Ankles with poor mobility that lack dorsiflexion ROM as a result of tight soleus, gastrocnemius, and tibialis posterior muscles could be one cause (Kritz et al., 2009). Another thing that may lead to this compensation might be instability of the foot as they might come up to the ball of the foot to help balance them and keep them from falling forward (Kritz et al., 2009). Implications from heels lifting off the floor at the bottom of a squat include compensation in other parts of the body such as the knees, hips, & lumbar spine that may lead to implications previously described. It could also cause instability of the knee joint (Kritz et al., 2009). Furthermore, it affects the ability to execute a well-balanced controlled squat (Kritz et al., 2009).

All in all, squats are an awesome exercise and are great for the booty. So use proper squat form & it like it’s hott. Because no one ever wrote a song about small butts.
References
Czaprowski, D., Biernat, R., & Kędra, A. (2012). Squat – rules of performing and most common mistakes. Polish Journal of Sport and Tourism, 19(1), 3-7. doi:10.2478/v10197-012-0001-6
Escamilla, R. F. (2001). Knee biomechanics of the dynamic squat exercise. Medicine and Science in Sports and Exercise [H.W. Wilson – EDUC], 33(1), 127.
Kritz, M., Cronin, J., & Hume, P. (2009). The bodyweight squat: A movement screen for the squat pattern. Strength and Conditioning Journal, 31(1), 76.
McGill, S. (2010). Core training: Evidence translating to better performance and injury prevention. Strength and Conditioning Journal, 32(3), 33-46. doi:10.1519/SSC.0b013e3181df4521
Myer, G. D., Kushner, A. M., Brent, J. L., Schoenfeld, B. J., Hugentobler, J., Lloyd, R. S.. . McGill, S. M. (2014). The back squat: A proposed assessment of functional deficits and technical factors that limit performance. Strength and Conditioning Journal, 36(6), 4-27. doi:10.1519/SSC.0000000000000103